







Clinical and medical
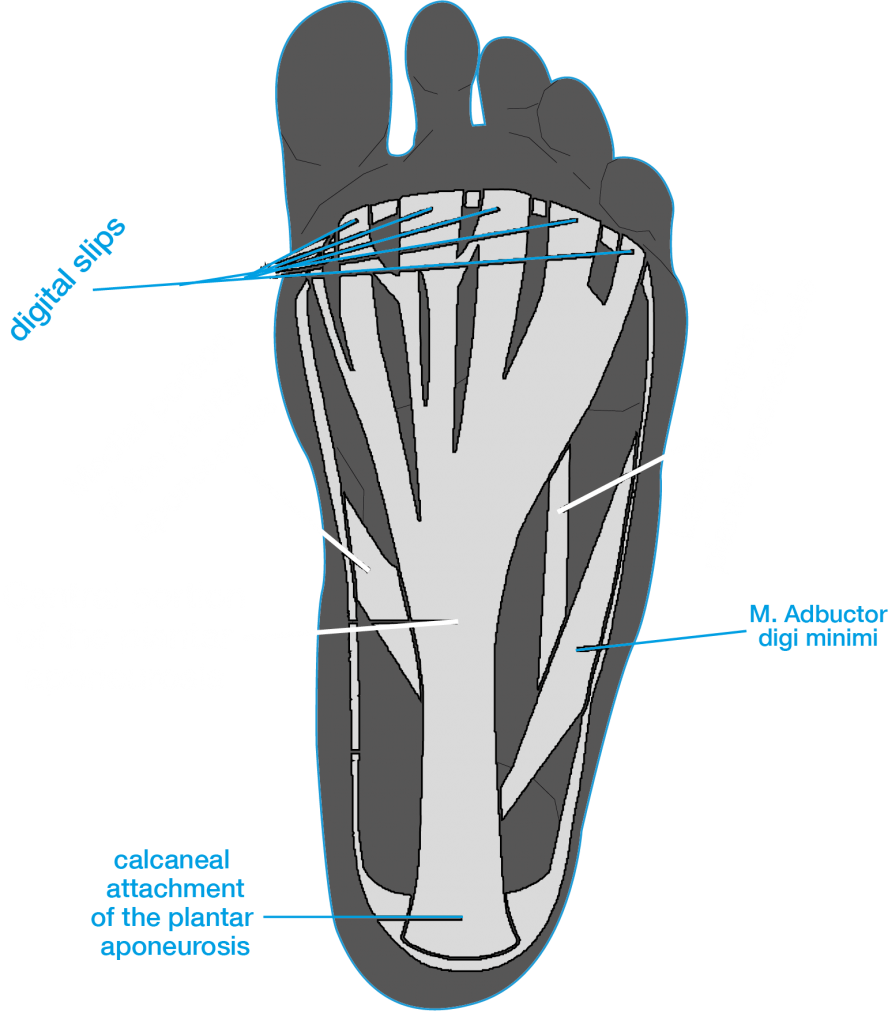
6 things you should know about plantar fasciitis
Share on facebook Facebook Share on twitter Twitter Share on google Google+ Share on email Email Plantar fasciitis (PF) is an overuse injury characterised by
Share on facebook Facebook Share on twitter Twitter Share on google Google+ Share on email Email Plantar fasciitis (PF) is an overuse injury characterised by
